Ollie the Very Happy Cavalier King Charles Spaniel, A Case Study: Meningoencephalitis of Unknown Etiology (MUE)
MUE refers to a category of conditions where the central nervous system becomes the target of inflammatory cell infiltration. While this immune-mediated attack on the brain and spinal cord is frequently observed in small-breed dogs—often hinting at an underlying genetic link—large-breed patients are also susceptible. Typically, we begin to see these clinical signs in pets that have reached at least six months of age.

Ollie’s Story: Recognizing the Signs of MUE
In June 2024, Oliver (“Ollie”), a three-year-old Cavalier King Charles Spaniel, presented to VNIoC exhibiting severe clinical signs of cervical distress. His discomfort was profound, manifesting as an inability to maintain normal head carriage. The pain was debilitating enough to silence his characteristic "happy bark," a cherished interaction with his owner. Furthermore, Ollie experienced involuntary muscle spasms and vocalized in distress while attempting to escape the localized sensation. His family observed a marked shift in his demeanor, noting he had become significantly lethargic and withdrawn. Due to the severity of these symptoms, Ollie required assistance and was being carried up and down the stairs.
Our clinical examination corroborated these findings, revealing proprioceptive deficits such as paw scuffing and mild ataxia. Additionally, he showed intense resistance to any voluntary range of motion in his neck.
Given the progression of his history and physical signs, we advised moving forward with advanced diagnostics, specifically a magnetic resonance imagining (MRI) scan of the cervical spine and a cerebrospinal fluid (CSF) analysis to further investigate the underlying cause.
Diagnosing Meningoencephalitis of Unknown Etiology (MUE)
Promptly after his clinical assessment, we conducted an MRI evaluation of Ollie's cervical spine and obtained a cerebrospinal fluid sample for detailed laboratory study.
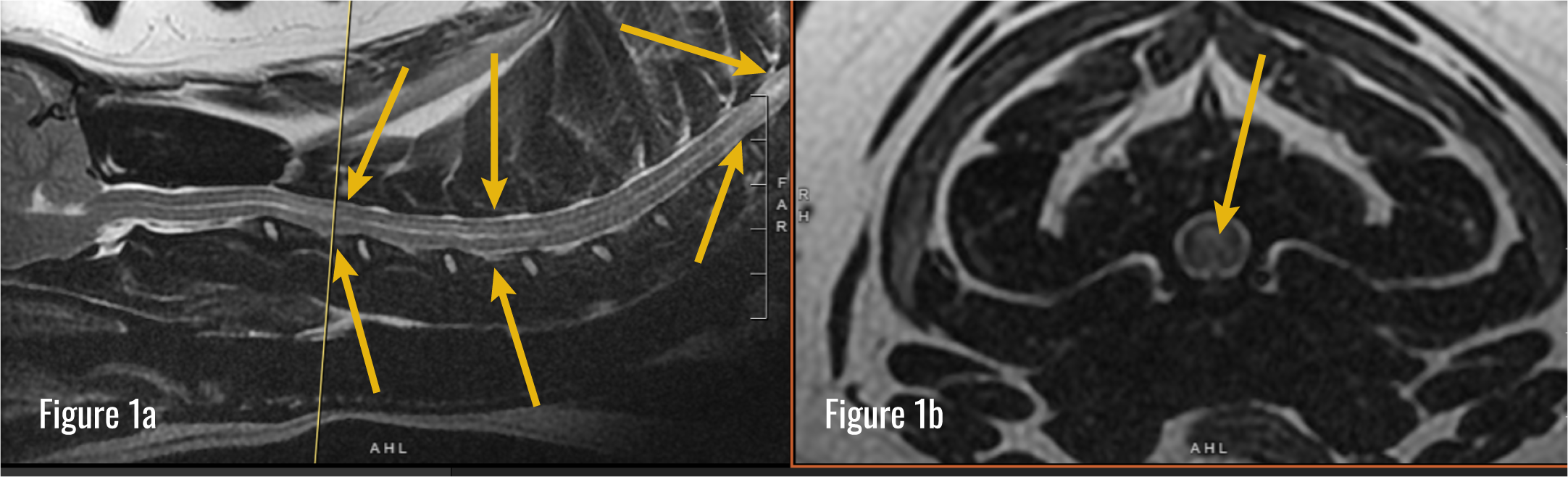
Figure 1a – Sagittal T2W image of Ollie’s neck. His head is to the left and his shoulders are to the right. Arrows point where the spinal cord is swollen and has areas of inflammation and edema.
Figure 1b – Axial T2W image of Ollie’s neck. This slice is taken from the area marked with the yellow line in Figure 1a. The area points to where the swollen spinal cord has areas of inflammation and edema.
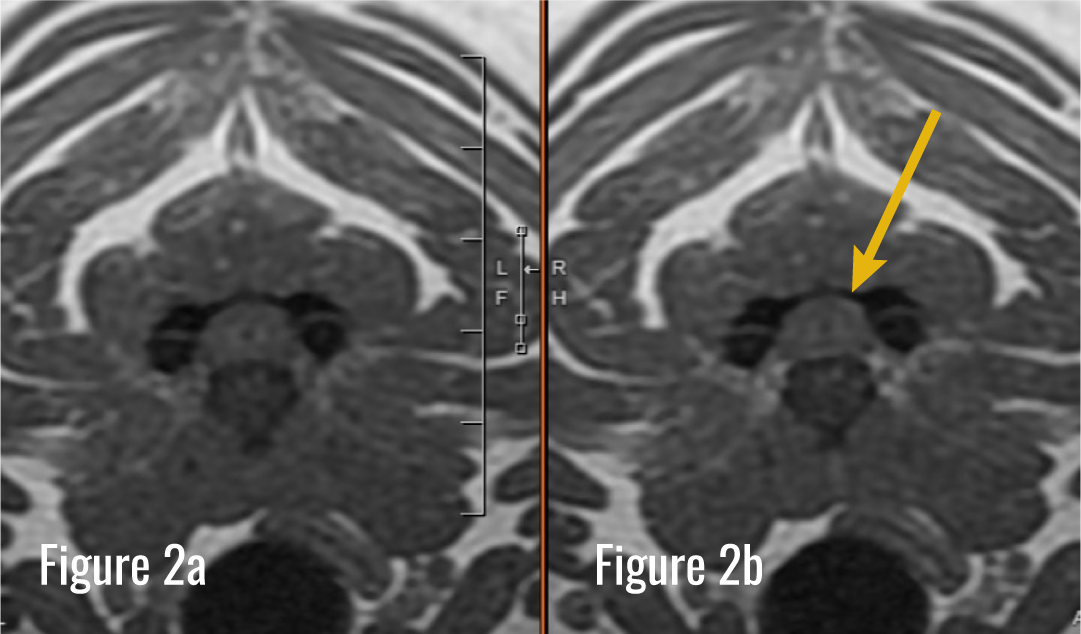
Figure 2a – Axial T1W image of Ollie’s neck.
Figure 2b – Axial T1W with contrast image of Ollie’s neck. The arrow points to an area of increased enhancement indicative of inflammation.
The imaging results revealed significant abnormalities, specifically multi-focal regions of inflammation and edema within the middle and lower cervical segments that demonstrated contrast enhancement. Although a Chiari-like malformation was identified—a congenital finding frequently noted in this breed—it was determined not to be the primary source of his acute neurological distress.
Analysis of the fluid collection showed marked pleocytosis and elevated protein concentrations. The cellular population consisted of a mixed inflammatory infiltrate including lymphocytes, macrophages, and neutrophils; however, no fungal or bacterial organisms were detected. A rigorous screening for neoplastic cells also returned negative results.
By integrating these diagnostic findings and systematically excluding alternative etiologies, we established a presumptive diagnosis of MUE.
In instances where the fluid analysis suggests a septic or fungal process, further cultures and systemic infectious disease panels are warranted. As Ollie’s initial indicators were inconsistent with such pathologies, these additional diagnostic avenues were not pursued.
Clinical Note: While a definitive confirmation of MUE requires an invasive brain tissue biopsy, the associated risks and financial implications often lead to a presumptive diagnosis based on a combination of advanced imaging, fluid analysis, and the exclusion of other inflammatory triggers.
Cause of MUE in Dogs
The precise etiology of MUE remains elusive. This pathology is characterized by the infiltration of the central nervous system by inflammatory cells, and within the clinical community, it is broadly recognized as an immune-mediated or autoimmune process.
It is hypothesized that the development of MUE involves a multifactorial interplay of the following elements:
Immune System Dysregulation: The patient's natural defenses erroneously target neural tissues as foreign threats, triggering an aggressive inflammatory cascade within the brain and spine.
Genetic Susceptibility: A hereditary component is often suspected, particularly in toy and small-breed dogs such as Maltese, Pugs, Chihuahuas, and Yorkshire Terriers.
Potential Environmental Catalysts: Factors such as viral exposure, recent immunizations, or existing systemic inflammation may serve as triggers that activate this pathological immune response in predisposed individuals.
Cytosar Treatment for Dogs with MUE
Given that the underlying pathology involves a hyperactive immune response, therapeutic strategies generally necessitate lifelong administration of immunosuppressive or immunomodulating agents to halt the patient's natural defenses from targeting neural tissues. Certain protocols incorporate chemotherapeutic agents designed to inhibit rapidly dividing cellular populations. Frequently, our clinical approach includes utilizing immunosuppressive concentrations of corticosteroids alongside medications specifically selected for their efficacy in traversing the blood-brain barrier.
Management is typically permanent and involves consistent serial evaluations with a neurologist. Periodic diagnostic retesting is often warranted to monitor the effectiveness of the intervention. Successful long-term management aims to enhance the patient's quality of life while significantly extending the period of disease-free progression.
For Ollie's therapeutic protocol, we initiated a regimen of immunosuppressive prednisone alongside Cytosar, a chemotherapeutic agent. This intervention began with a continuous 24-hour intravenous infusion, followed by subsequent outpatient administrations initiated on a four-week cycle.
In some instances, a recrudescence of clinical signs may necessitate modifications to the chemotherapy intervals. Such a deviation occurred only once for Ollie, approximately twelve months into his management plan. Furthermore, he remains on supplemental medications at home to maintain stability between clinical visits.



MUE Prognosis and Long-Term Management
Although clinical outcomes vary based on the specific pathology, patients demonstrating a positive therapeutic response beyond the six-month mark—a milestone Ollie successfully achieved—often carry a more favorable long-term outlook compared to those who fail to stabilize during the initial phase of intervention.
We are pleased to share that Ollie has maintained neurological stability following a single episode of symptom recurrence and subsequent refinement of his chemotherapy intervals and home maintenance protocols.